An award-winning cannabis podcast for women, by women. Hear joyful stories and useful advice about cannabis for health, well-being, and fun—especially for needs specific to women like stress, sleep, and sex. We cover everything from: What’s the best weed for sex? Can I use CBD for menstrual cramps? What are the effects of the Harlequin strain or Gelato strain? And, why do we prefer to call it “cannabis” instead of “marijuana”? We also hear from you: your first time buying legal weed, and how ...
…
continue reading
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://podcastplayer.com/legal.
Similar to PulmPEEPs
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Are you looking for more happiness, success and vitality in your life? Get inspired each week with wellness and performance expert, Integrative Medicine Fellow, author & keynote speaker, Kristel Bauer. Live Greatly shares empowering conversations and insights about happiness, wellness & success to support your personal and professional development. Kristel talks with top experts, leaders and inspiring individuals to help you embrace a growth mindset and excel in your work/life. Kristel then ...
…
continue reading
Being positive is up to you. When you understand how your mind works, you really can create the life you desire.
…
continue reading
AnthroPod is produced by the Society for Cultural Anthropology. In each episode, we explore what anthropology teaches us about the world and people around us.
…
continue reading
Named by Oprah as a thought leader for the next generation and one of Inc.’s 500 fastest growing companies, Marie Forleo’s goal is to help you become the person you most want to be. In this show, Marie and her guests share actionable strategies for greater happiness, success, motivation, creativity, productivity, love, health, contribution and fulfillment — often with a lot of laughs. From business, marketing and career advice, to tackling failure, disappointment and fear, to philanthropy an ...
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Learn French with free daily podcasts, brought to you by French teachers from Paris. Hébergé par Acast. Visitez acast.com/privacy pour plus d'informations.
…
continue reading
(Apple's Best of 2018) In-depth conversations with people at the top of their game. Jordan Harbinger unpacks guests' wisdom into practical nuggets you can use to impact your work, life, and relationships. Learn from leaders (Ray Dalio, Simon Sinek, Mark Cuban), entertainers (Moby, Tip "T.I." Harris, Dennis Quaid), scientists (Neil deGrasse Tyson, Bill Nye), athletes (Kobe Bryant, Dennis Rodman, Tony Hawk) and an eclectic array of fascinating minds, from art forgers and arms traffickers to sp ...
…
continue reading
BackStory is a weekly public podcast hosted by U.S. historians Ed Ayers, Brian Balogh, Nathan Connolly and Joanne Freeman. We're based in Charlottesville, Va. at Virginia Humanities. There’s the history you had to learn, and the history you want to learn - that’s where BackStory comes in. Each week BackStory takes a topic that people are talking about and explores it through the lens of American history. Through stories, interviews, and conversations with our listeners, BackStory makes histo ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
107. Fellows’ Case Files: University of Kansas Medical Center KUMC
Manage episode 509430687 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://podcastplayer.com/legal.
After a brief hiatus, we are excited to be back today with another Fellows’ Case Files! Today we’re virtually visiting the University of Kansas Medical Center (KUMC) to hear about a fascinating pulmonary presentation. There are some fantastic case images and key learning points. Take a listen and see if you can make the diagnosis along with us. As always, let us know your thoughts and definitely reach out if you have an interesting case you’d like to share.
Meet Our Guests
Dr. Vishwajit Hegde completed his internal medicine residency at University of Kansas Medical Center where he stayed for fellowship and is currently a second year Pulmonary and Critical Care medicine fellow.
Dr. Sahil Pandya is an Associate Professor of Medicine and Program Director of the PCCM Fellowship at KUMC.
Case Presentation
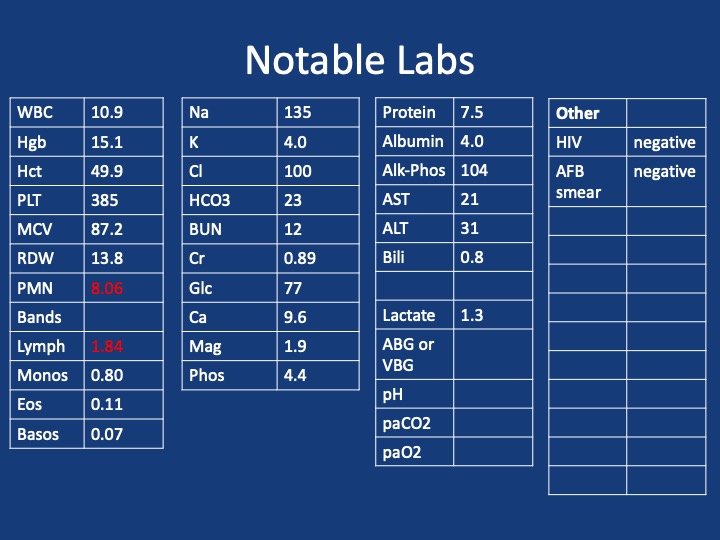
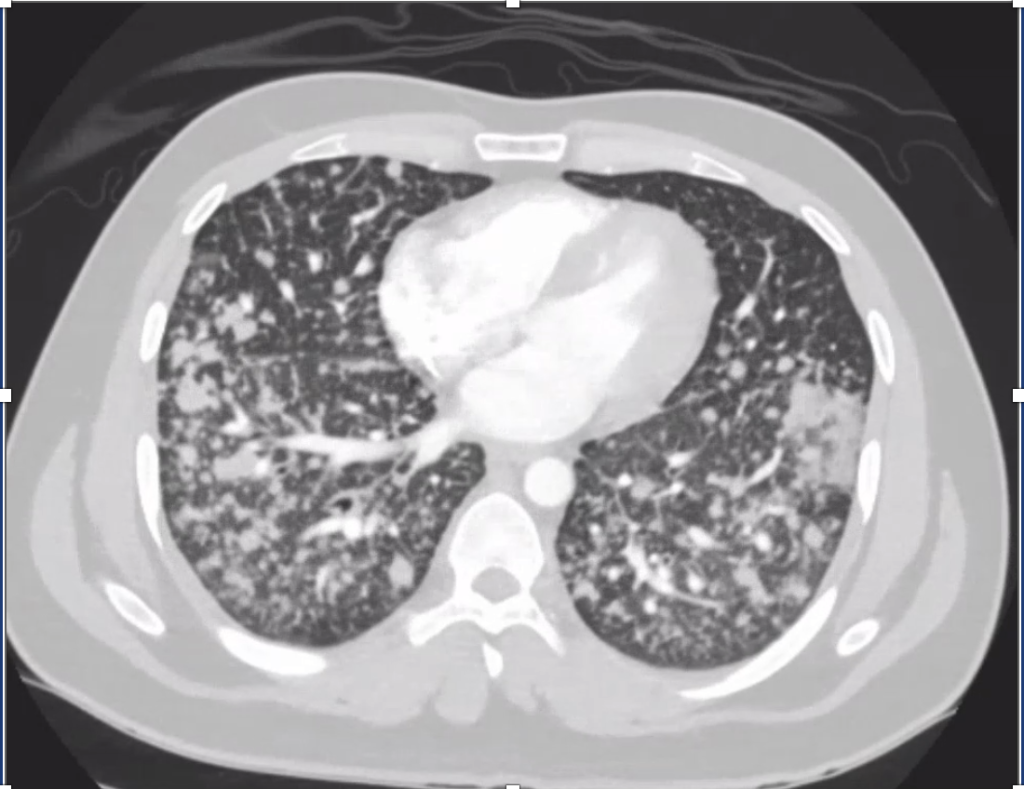
Imaging



Infographic
Key Learning Points
1) Initial frame & diagnostic mindset
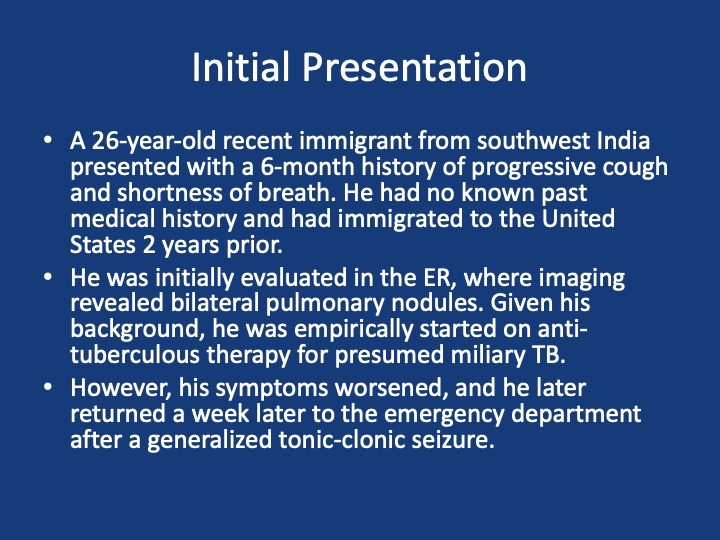
- Young (26), subacute → chronic dyspnea/cough with diffuse pulmonary nodules; avoid premature closure on TB.
- Use a Bayesian approach: combine pre-test probability (epidemiology, exposures, tempo) with targeted tests to decide next steps.
- Always confirm TB when possible (micro/path + resistance testing); empiric RIPE may be reasonable but shouldn’t replace tissue when stakes are high.
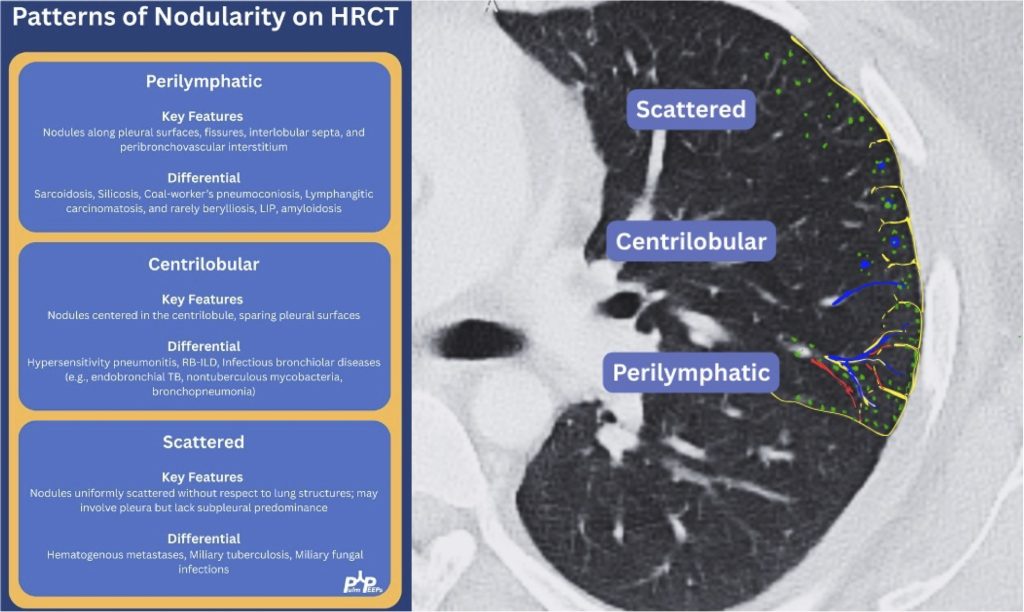
2) Imaging pearls—nodular pattern recognition
- Ask three things: craniocaudal distribution, symmetry, central vs peripheral.
- Centrilobular (spares pleura/fissures): airway-centered (e.g., NTM, bronchiolitis, tree-in-bud).
- Perilymphatic (tracks fissures/pleura & septa): sarcoid, lymphangitic spread.
- Random/diffuse (involves pleural surfaces): hematogenous spread → think miliary TB, disseminated fungal, septic emboli, metastatic disease.
- Interval change matters: new cavitation and confluence can upweight infection or aggressive malignancy.
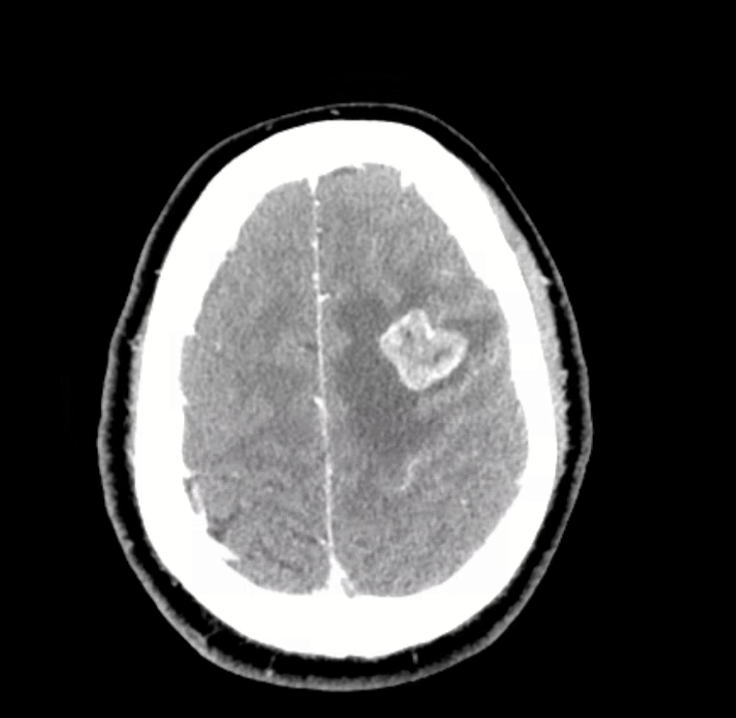
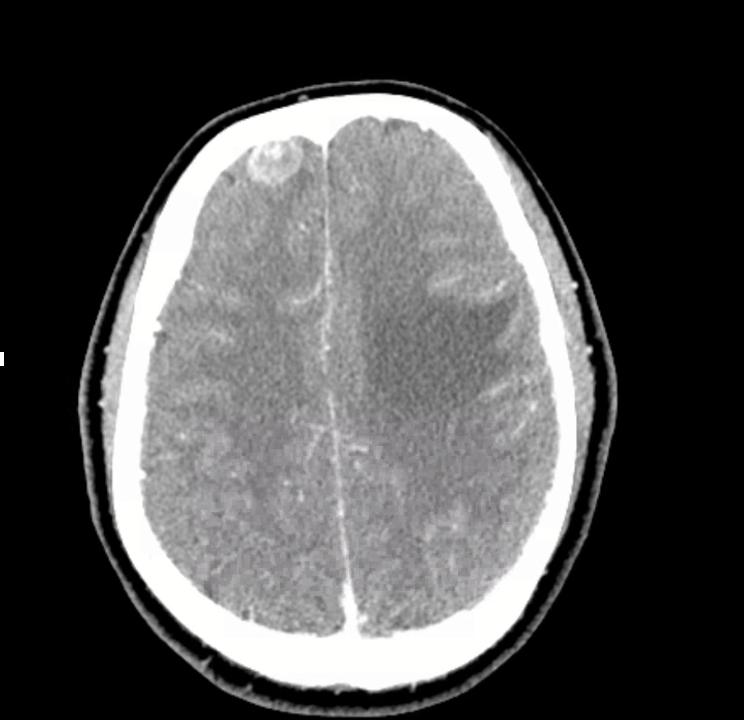
3) Neuro findings—ring-enhancing lesions
- Differential: septic emboli/abscess, nocardia, fungal, TB, parasites, metastases, vasculitis, sarcoid.
- Partner with neuroradiology for pattern nuances; treat seizures but keep searching for the unifying diagnosis.
4) Lab/serology strategy
- Broad infectious workup (AFB × multiple, fungal serologies), HIV and basic immune screen.
- Negative/indeterminate tests don’t end the search—revisit history (e.g., Ohio travel → histo/blasto risk).
5) “Tissue is the issue”—choosing the procedure
- For diffuse nodules with mediastinal adenopathy and stable patient: EBUS-TBNA + BAL, consider transbronchial or cryobiopsy.
- Cryobiopsy pros: larger, less crush artifact, better for molecular testing; cons: ↑ bleeding/pneumothorax vs forceps.
- VATS still best for certain ILD questions or if less invasive routes are non-diagnostic—but weigh patient preference and stage/likelihood of yield.
6) ROSE (rapid on-site evaluation) in bronchoscopy
- Confirms adequacy in real time, steers you away from necrotic zones, helps decide when you’ve got enough for molecular studies, and when to pivot sites—reduces anesthesia time and repeat procedures.
7) Final diagnosis & management
- Path: TTF-1+, CK7+, napsin A → pulmonary adenocarcinoma with a fusion driver.
- Therapy: Targeted TKI (crizotinib) → dramatic radiographic response of miliary lung disease and CNS lesions.
- Teaching point: even “miliary TB-like” lungs + CNS lesions in a 20-something can be driver-positive lung cancer—don’t let age or pattern blind you.
References and Further Reading
- Desai, S., Devaraj, A., Lynch, D., & Sverzellati, N. (2020). Webb, Müller and Naidich’s high-resolution CT of the lung (6th ed.). Lippincott Williams & Wilkins.
- Rajeswaran, G., Becker, J. L., Michailidis, C., Pozniak, A. L., & Padley, S. P. G. (2006). The radiology of IRIS (immune reconstitution inflammatory syndrome) in patients with mycobacterial tuberculosis and HIV co-infection: appearances in 11 patients. Clinical radiology, 61(10), 833-843
- Poletti, V., Ravaglia, C., & Tomassetti, S. (2016). Transbronchial cryobiopsy in diffuse parenchymal lung diseases. Current opinion in pulmonary medicine, 22(3), 289-296.
- Norman, G. R., Monteiro, S. D., Sherbino, J., Ilgen, J. S., Schmidt, H. G., & Mamede, S. (2017). The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 92(1), 23-30.
107 episodes
Manage episode 509430687 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://podcastplayer.com/legal.
After a brief hiatus, we are excited to be back today with another Fellows’ Case Files! Today we’re virtually visiting the University of Kansas Medical Center (KUMC) to hear about a fascinating pulmonary presentation. There are some fantastic case images and key learning points. Take a listen and see if you can make the diagnosis along with us. As always, let us know your thoughts and definitely reach out if you have an interesting case you’d like to share.
Meet Our Guests
Dr. Vishwajit Hegde completed his internal medicine residency at University of Kansas Medical Center where he stayed for fellowship and is currently a second year Pulmonary and Critical Care medicine fellow.
Dr. Sahil Pandya is an Associate Professor of Medicine and Program Director of the PCCM Fellowship at KUMC.
Case Presentation
Imaging
Infographic
Key Learning Points
1) Initial frame & diagnostic mindset
- Young (26), subacute → chronic dyspnea/cough with diffuse pulmonary nodules; avoid premature closure on TB.
- Use a Bayesian approach: combine pre-test probability (epidemiology, exposures, tempo) with targeted tests to decide next steps.
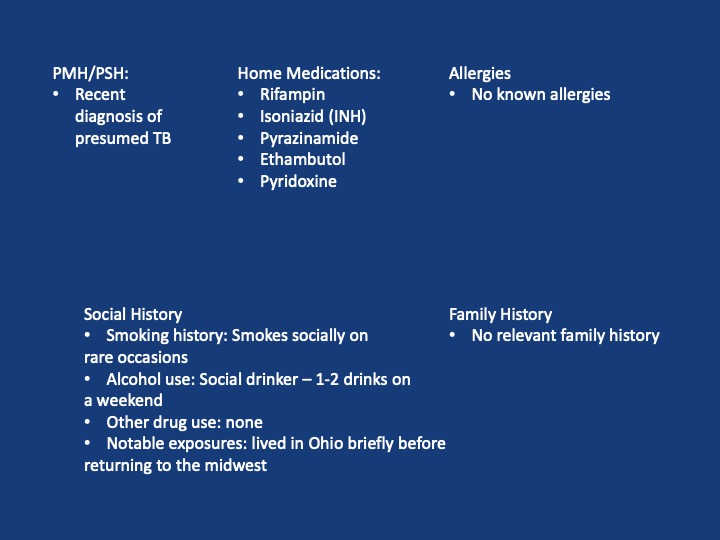
- Always confirm TB when possible (micro/path + resistance testing); empiric RIPE may be reasonable but shouldn’t replace tissue when stakes are high.
2) Imaging pearls—nodular pattern recognition
- Ask three things: craniocaudal distribution, symmetry, central vs peripheral.
- Centrilobular (spares pleura/fissures): airway-centered (e.g., NTM, bronchiolitis, tree-in-bud).
- Perilymphatic (tracks fissures/pleura & septa): sarcoid, lymphangitic spread.
- Random/diffuse (involves pleural surfaces): hematogenous spread → think miliary TB, disseminated fungal, septic emboli, metastatic disease.
- Interval change matters: new cavitation and confluence can upweight infection or aggressive malignancy.
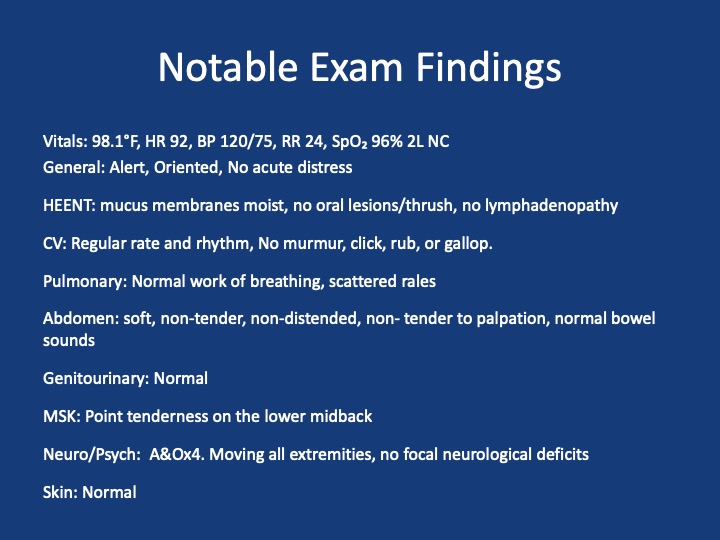
3) Neuro findings—ring-enhancing lesions
- Differential: septic emboli/abscess, nocardia, fungal, TB, parasites, metastases, vasculitis, sarcoid.
- Partner with neuroradiology for pattern nuances; treat seizures but keep searching for the unifying diagnosis.
4) Lab/serology strategy
- Broad infectious workup (AFB × multiple, fungal serologies), HIV and basic immune screen.
- Negative/indeterminate tests don’t end the search—revisit history (e.g., Ohio travel → histo/blasto risk).
5) “Tissue is the issue”—choosing the procedure
- For diffuse nodules with mediastinal adenopathy and stable patient: EBUS-TBNA + BAL, consider transbronchial or cryobiopsy.
- Cryobiopsy pros: larger, less crush artifact, better for molecular testing; cons: ↑ bleeding/pneumothorax vs forceps.
- VATS still best for certain ILD questions or if less invasive routes are non-diagnostic—but weigh patient preference and stage/likelihood of yield.
6) ROSE (rapid on-site evaluation) in bronchoscopy
- Confirms adequacy in real time, steers you away from necrotic zones, helps decide when you’ve got enough for molecular studies, and when to pivot sites—reduces anesthesia time and repeat procedures.
7) Final diagnosis & management
- Path: TTF-1+, CK7+, napsin A → pulmonary adenocarcinoma with a fusion driver.
- Therapy: Targeted TKI (crizotinib) → dramatic radiographic response of miliary lung disease and CNS lesions.
- Teaching point: even “miliary TB-like” lungs + CNS lesions in a 20-something can be driver-positive lung cancer—don’t let age or pattern blind you.
References and Further Reading
- Desai, S., Devaraj, A., Lynch, D., & Sverzellati, N. (2020). Webb, Müller and Naidich’s high-resolution CT of the lung (6th ed.). Lippincott Williams & Wilkins.
- Rajeswaran, G., Becker, J. L., Michailidis, C., Pozniak, A. L., & Padley, S. P. G. (2006). The radiology of IRIS (immune reconstitution inflammatory syndrome) in patients with mycobacterial tuberculosis and HIV co-infection: appearances in 11 patients. Clinical radiology, 61(10), 833-843
- Poletti, V., Ravaglia, C., & Tomassetti, S. (2016). Transbronchial cryobiopsy in diffuse parenchymal lung diseases. Current opinion in pulmonary medicine, 22(3), 289-296.
- Norman, G. R., Monteiro, S. D., Sherbino, J., Ilgen, J. S., Schmidt, H. G., & Mamede, S. (2017). The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 92(1), 23-30.
107 episodes
All episodes
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to PulmPEEPs
An award-winning cannabis podcast for women, by women. Hear joyful stories and useful advice about cannabis for health, well-being, and fun—especially for needs specific to women like stress, sleep, and sex. We cover everything from: What’s the best weed for sex? Can I use CBD for menstrual cramps? What are the effects of the Harlequin strain or Gelato strain? And, why do we prefer to call it “cannabis” instead of “marijuana”? We also hear from you: your first time buying legal weed, and how ...
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Are you looking for more happiness, success and vitality in your life? Get inspired each week with wellness and performance expert, Integrative Medicine Fellow, author & keynote speaker, Kristel Bauer. Live Greatly shares empowering conversations and insights about happiness, wellness & success to support your personal and professional development. Kristel talks with top experts, leaders and inspiring individuals to help you embrace a growth mindset and excel in your work/life. Kristel then ...
…
continue reading
Being positive is up to you. When you understand how your mind works, you really can create the life you desire.
…
continue reading
AnthroPod is produced by the Society for Cultural Anthropology. In each episode, we explore what anthropology teaches us about the world and people around us.
…
continue reading
Named by Oprah as a thought leader for the next generation and one of Inc.’s 500 fastest growing companies, Marie Forleo’s goal is to help you become the person you most want to be. In this show, Marie and her guests share actionable strategies for greater happiness, success, motivation, creativity, productivity, love, health, contribution and fulfillment — often with a lot of laughs. From business, marketing and career advice, to tackling failure, disappointment and fear, to philanthropy an ...
…
continue reading
The Voice of ASWJ Australia. Listen to & Download Our Latest Programs. Topics: Aqeedah (Creed), Tafsir Qur'an, Islamic Fiqh, History, Youth & Community programs, Medical & Health programs and much much more. Podcasts are in Arabic & English.
…
continue reading
Learn French with free daily podcasts, brought to you by French teachers from Paris. Hébergé par Acast. Visitez acast.com/privacy pour plus d'informations.
…
continue reading
(Apple's Best of 2018) In-depth conversations with people at the top of their game. Jordan Harbinger unpacks guests' wisdom into practical nuggets you can use to impact your work, life, and relationships. Learn from leaders (Ray Dalio, Simon Sinek, Mark Cuban), entertainers (Moby, Tip "T.I." Harris, Dennis Quaid), scientists (Neil deGrasse Tyson, Bill Nye), athletes (Kobe Bryant, Dennis Rodman, Tony Hawk) and an eclectic array of fascinating minds, from art forgers and arms traffickers to sp ...
…
continue reading
BackStory is a weekly public podcast hosted by U.S. historians Ed Ayers, Brian Balogh, Nathan Connolly and Joanne Freeman. We're based in Charlottesville, Va. at Virginia Humanities. There’s the history you had to learn, and the history you want to learn - that’s where BackStory comes in. Each week BackStory takes a topic that people are talking about and explores it through the lens of American history. Through stories, interviews, and conversations with our listeners, BackStory makes histo ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!



